January 2012
Lisa A. Pitelka-Zengou, MD1, Xiaoqi Lin, MD, PhD1, Neil Mascarenhas, MD3, Julia Samolczyk, CT(ASCP) 2, Mark Wang, MD1
- Department of Cytopathology, Northwestern University, Feinberg School of Medicine, Chicago
- Northwestern Memorial Hospital, Chicago, IL, USA
- Department of Interventional Radiology, Northwestern Memorial Hospital, Chicago, IL, USA
Case History:
A 35 year-old woman presented with a two-month history of right lower quadrant abdominal pain which increased with activities such as exercise and movement, as well as during menses. Her past medical history was significant for cerebral palsy and irritable bowel syndrome. A CT scan performed at an outside hospital revealed a 1.7 cm soft tissue mass in the subcutaneous tissue of the right abdomen. On physical exam, the mass was non-mobile, firm, painful to palpation, and did not change with Valsalva or leg lift. The mass was just superior to her Pfannenstiel scar from a Cesarean section. Ultrasound further showed a hypoechoic, mildly lobulated, solid, heterogeneous nodule measuring 2.0 x 1.8 x 1.3 cm, in contact with the fascia of the rectus muscle (Fig 1). The mass demonstrated internal vascularity by Doppler. The radiological differential diagnosis included a desmoid tumor, endometrioma, metastatic carcinoma, or sarcoma.
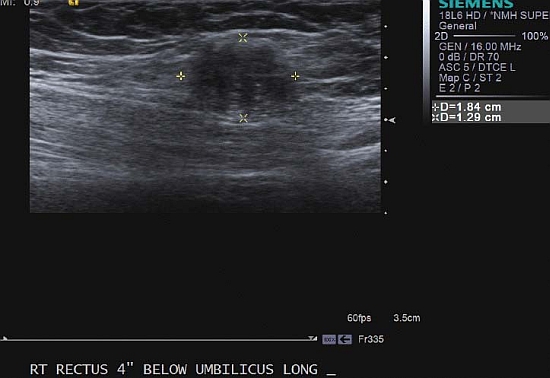 |
| Fig. 1 Ultrasound image |
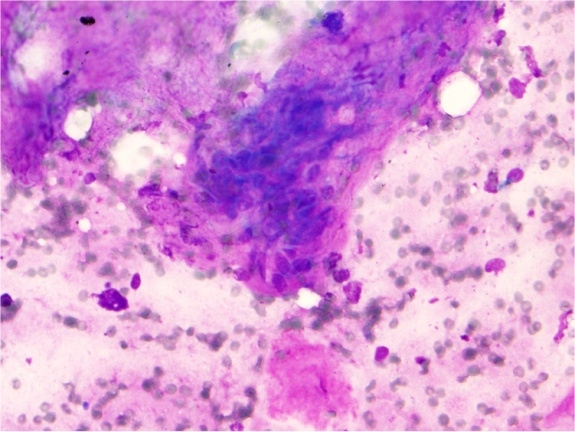 |
| Fig. 2 DQ-stained FNA |
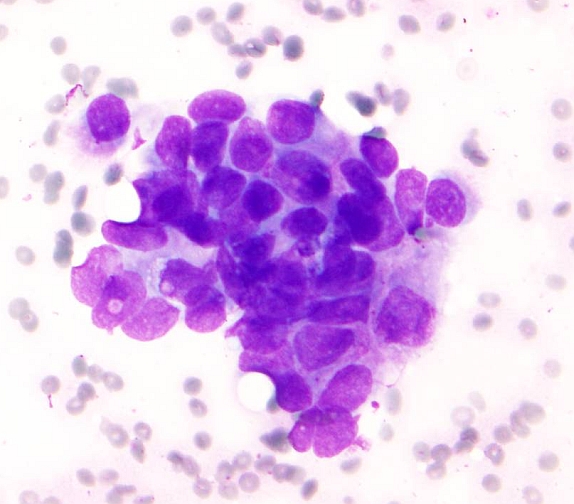 |
| Fig. 3 DQ stained touch preparation |
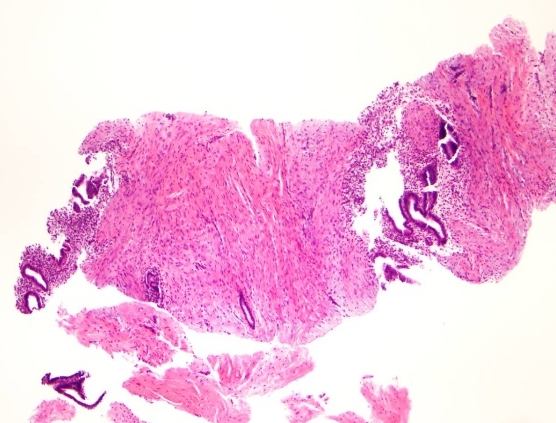 |
| Fig. 4a H&E-stained core biopsy |
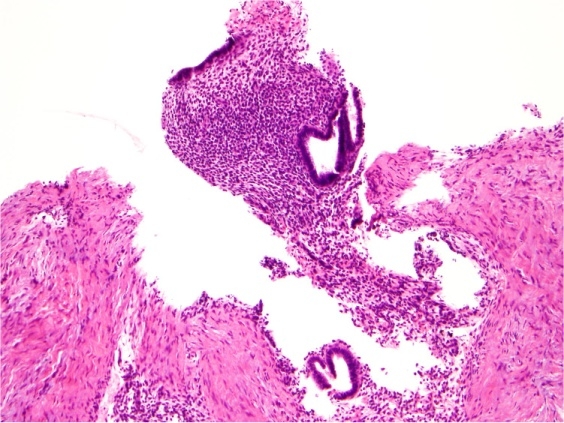 |
| Fig. 4b H&E-stained core biopsy |
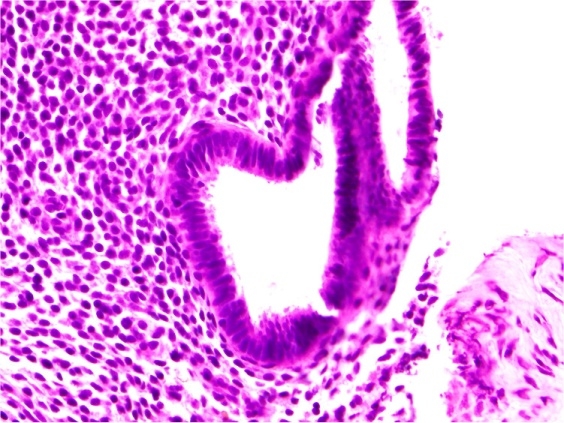 |
| Fig. 4c H&E-stained core biopsy |
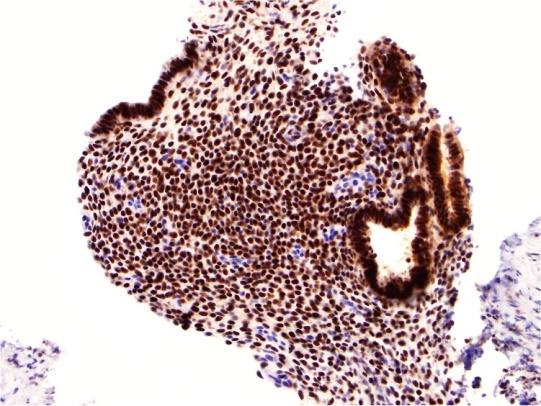 |
| Fig. 5 IHC Estrogen Receptor |
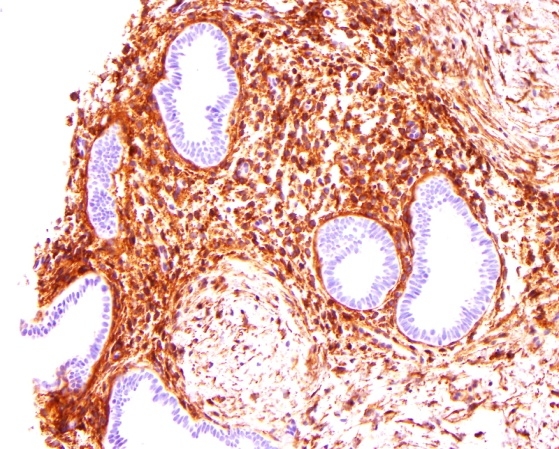 |
| Fig. 6 IHC CD10 |
Your diagnosis?