April 2013
Authors: Rubina Cocker, MD1; Cecilia Gimenez, MD 1; and Walid E. Khalbuss, MD PhD FIAC2
1 North Shore-Long Island Jewish Health System, Lake Success, New York; USA; 2 University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania USA.
Reviewer: Manon Auger MD; McGill Univ Health Center; Department of Pathology; Montreal, QC; Canada Clinical
History: An 82 year old male presented with complaints of progressive dysphagia and hoarseness for a few weeks. The patient was noted to be status post partial glossectomy with bilateral neck dissection and radiation therapy for a base of tongue squamous cell carcinoma. PET/ CT scan revealed multiple lesions in the right subglottis and trachea. An endobronchial ultrasound guided FNA biopsy of the tracheal lesion was performed. Representative images are provided: DQ stain (Images 1 & 2). Pap stain (Image 3), Cell block, H&E stain (Image 4), and Immunostain of p16 and HPV ISH (image 5).
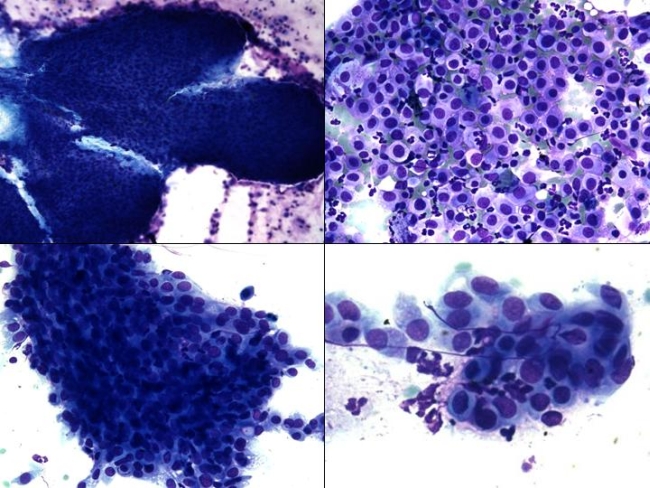 |
| Image 1: DQ stain, left upper x100, left lower, x200, right upper x300, and right lower, x600. |
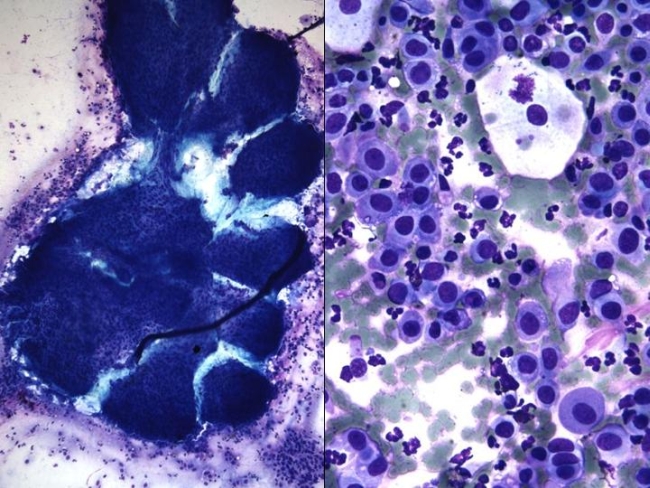 |
| Image 2: DQ stain, left, x100, right, x 600. |
 |
| Image 3: Papanicolau stain, x 600. |
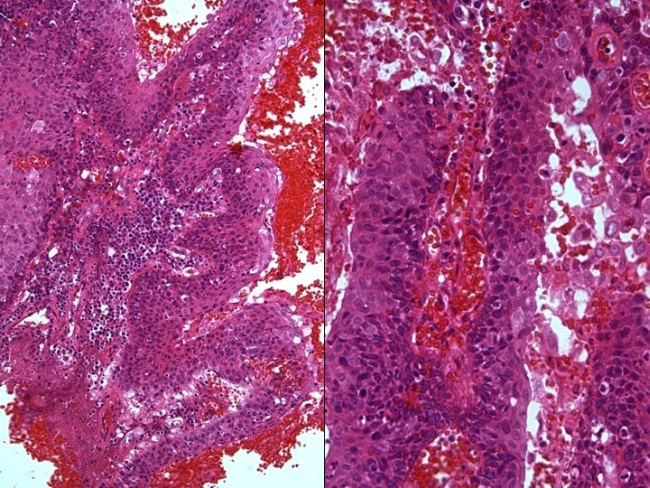 |
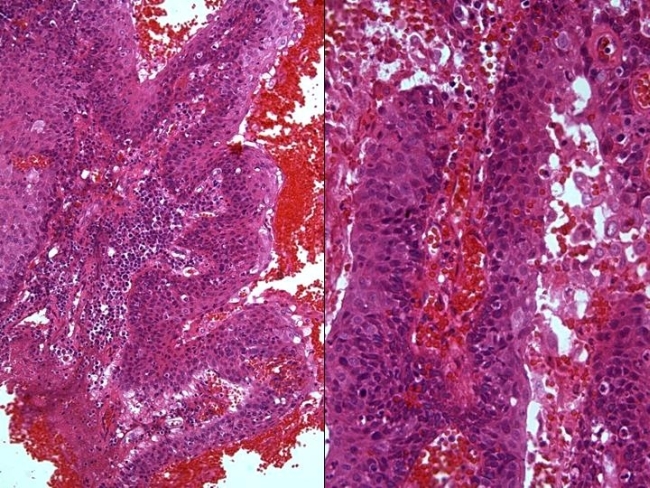
| Image 4: Cell block, H&E Left, x 400 and right, x 200. |
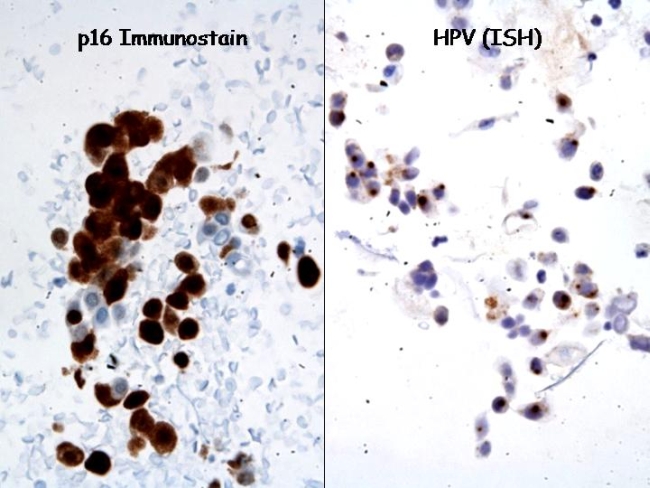 |
| Image 5: Immunostain of p16 (nuclear staining, left, original magnification, x630).) and In situ hybridization for high-risk types of human Papillomavirus (ISH HPV, right) performed on the cell block. The signal is seen as punctuated dots within the nuclei of tumor cells (original magnification, x400). |